
Suspect an aortic dissection in patients with chest pain plus any of the following:
- New neurological problems
- Anterior spinal artery infarction with loss of motor function and loss of sensation (with preserved position and vibratory senses)
- Oculosympathetic paresis, or Horner syndrome, with miosis, ptosis, and anhidrosis
- A painful Horner’s is a dissection until proven otherwise
- Acute renal infarction (flank pain and hematuria, along with a noncontrast CT of the abdomen and pelvis that is negative for ureterolithiasis)
- Acute mesenteric ischemia (sudden onset of severe abdominal pain that is out of proportion to physical examination findings, lactic acidosis)
- New murmur of aortic regurgitation (listen here; it is an early diastolic decrescendo murmur, best at left upper sternal border, louder with leaning forward or with increased afterload)
- Chest radiograph showing a widened mediastinum
- Ischemic limb (look for pulselessness, pallor, pain, paresthesias, paralysis & poikilothermia)
- New hoarseness or dysphasia
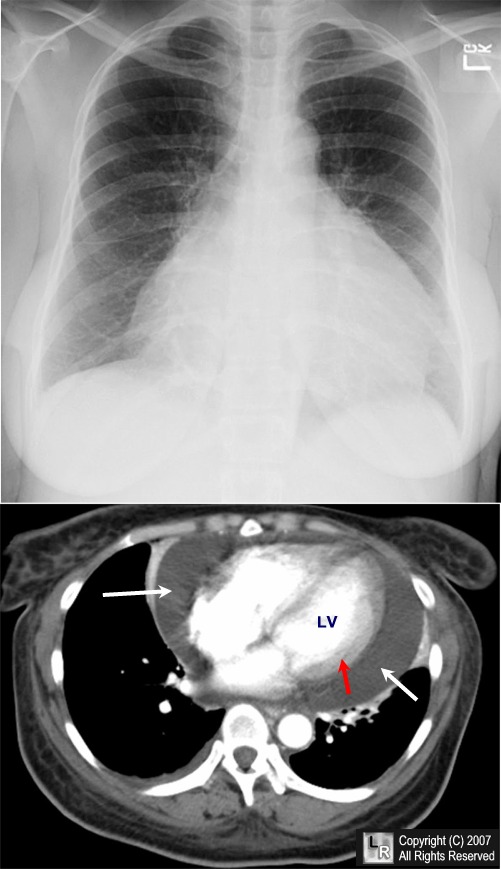
- Cardiac tamponade (↑ heart rate, ↑ neck veins, ↓ blood pressure, clear lungs)
- Unexplained pericardial effusion (distant heart sounds, electrical alternans and low voltage on electrocardiogram, chest radiograph with symmetrically enlarged cardiac silhouette)
- Evidence of a rare collagen vascular disease (e.g., Marfanoid habitus, hyperextensible joints)
References
- UpToDate (accessed 6/14/2013)
- Dennis, Mark, MBBS (2012). Mechanisms of Clinical Signs.
- Dahnert, Wolfgang, MD (2011). Radiology Review Manual, 7e.
- Fischer, Conrad, MD (2012). Master the Boards: USMLE Step 3, 2e.

{kind=link}
Leave a Reply