
The following is a comprehensive differential diagnosis and workup for seizures. The workup is (obviously!) not something that you have to do for every patient. You can, however, use the information below for standardized test preparation and to guide your thought process as you work up patients with seizures.
Please let me know if there’s anything that you might consider adding or changing.
Physical Examination
- Temperature (infection, febrile seizures, heat stroke, neuroleptic malignant syndrome, serotonin syndrome, TTP)
- Blood pressure (hypertensive encephalopathy, delirium tremens, eclampsia, sympathomimetic toxidrome, pheochromocytoma)
- Pulse (delirium tremens, sympathomimetic, anticholinergic toxidromes, e.g. TCA overdose)
- Pulse oximeter (hypoxemia)
- Neck for rigidity (meningitis, subarachnoid hemorrhage)
- Mental status (for hallucinations in delirium tremens)
- Skin for patches or contaminants (buprenorphine, organophosphates, etc.), petechiae (meningococcemia), jaundice, purpura (TTP), neurocutaneous syndromes (neurofibromatosis, tuberous sclerosis, Sturge-Weber syndrome)
Laboratory Studies
- Bedside fingerstick for glucose (hypoglycemia)
- WBC (infection, lithium toxicity)
- Hemoglobin and hematocrit (anemia, TTP-HUS)
- Platelets (chronic liver disease, TTP)
- Peripheral blood smear (schistocytes in TTP-HUS; basophilic stippling in lead poisoning)
- Serum glucose (to confirm bedside fingerstick for hypoglycemia, hyperglycemia)
- Serum sodium (hyponatremia or hypernatremia)
- Serum bicarbonate (uremia, alkalemia)
- BUN and creatinine (uremia, TTP-HUS)
- Calcium (hypocalcemia)
- Magnesium (hypomagnesemia)
- Phosphate (hypophosphatemia)
- Liver chemistry panel, ammonia, INR (liver failure, eclampsia, kernicterus, Reye Syndrome)
- Creatine kinase (for rhabdomyolysis)
- Serum osmolality and osmolal gap (hyperosmolarity, e.g. methanol, ethylene glycol, etc.)
- ABG (hypoxemia, hyperoxia (!), hypercapnia, alkalosis, anemia, carboxyhemoglobin, methemoglobinemia); not that a venous blood gas can be used instead of an arterial blood gas to rule out hypercapnia
- TSH (hyperthyroidism)
- Serum ethanol level (a high serum ethanol, suggests a diagnosis other than delirium tremens!)
- Blood cultures
- Urine
- urinalysis (infection, rhabdomyolysis, eclampsia, calcium oxalate crystal, porphyria)
- B-hCG (eclampsia)
- delta-aminolevulinic acid and porphobilinogen levels (acute intermittent porphyria)
- Lumbar puncture
- Subarachnoid hemorrhage
- Herpes Simplex Virus
- Varicella Zoster Virus
- Toxoplasmosis (immunocompromised patient with multiple ring-enhancing lesions on head CT; check serologies!)
- Cryptococcosis (immunocompromised patient with slowly-evolving, “mild” meningitis)
- Neurocysticercosis (patient from South America with a seizure and cystic lesion on brain imaging)
- Rickettsiosis
- Ehrlichiosis (tick exposure, hyperaminotransferasemia, thrombocytopenia, leukopenia, absence of rash, morulae on blood smear)
- West Nile virus
- Neurosyphilis
- Plasma free metanephrine, 24-hour urinary fractionated metanephrine and catecholamines (pheochromocytoma)
- Toxicology:
- Serum: osmolarity, ethanol, salicylates, theophylline, lithium, anti-epileptic drugs
- Arterial blood gas: carboxyhemoglobin, methemoglobin (per above), evidence of salicylate poisoning (respiratory alkalosis, metabolic acidosis, etc.)
- Urine: toxicology screen (cocaine, amphetamines, phencyclidine)
- Thick and thin peripheral blood smear (malaria, babesiosis)
- Anti-N-methyl-D-aspartate receptor (anti-NMDAR) antibodies (Anti-NMDA encephalitis)

Imaging
- Electrocardiogram – look for long QT interval (hypocalcemia), deep symmetrical T wave inversions (intracranial pathology) or the combination of tachycardia, wide QRS interval, rightward axis, and a tall R’ wave in aVR (tricyclic antidepressant cardiotoxicity)
- Chest radiograph (pneumonia, aspiration, salicylate-induced pulmonary edema)
- Brain CT (trauma, tumor, ischemia, intracranial bleed)
- Brain MRI
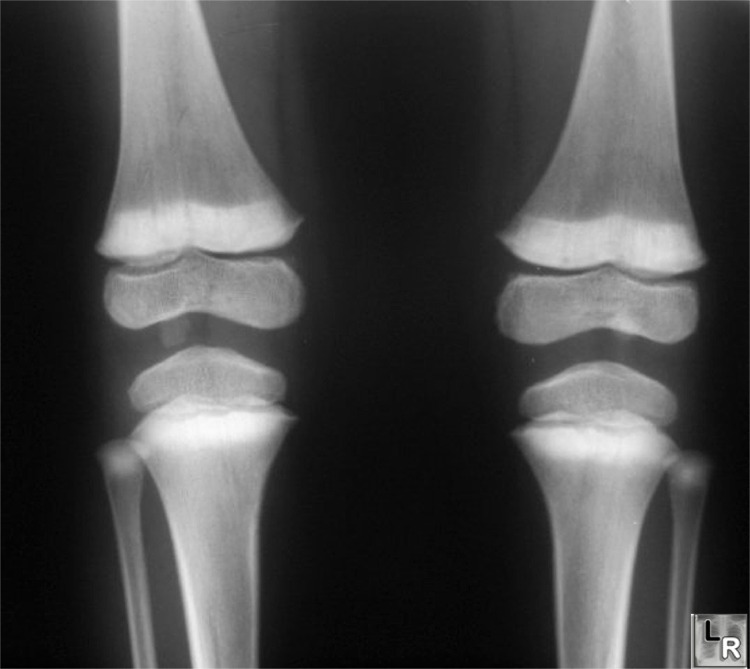
- “Lead lines” on knee radiographs
Other studies
- Electroencephalogram (EEG)
- Video monitoring (to rule out pseudoseizures)
- Upper endoscopy (Whipple’s disease)
Diagnostic/therapeutic drug challenges
- Pyridoxine (isoniazid toxicity)
- Magnesium (eclampsia)
Discontinue offenders:
- Antidepressants: bupropion, tricyclic antidepressants, venlafaxine
- Antihistamines: e.g., diphenhydramine
- Antimicrobials: chloroquine, hydroxychloroquine, imipenem-cilastatin, isoniazid
- Illicit drugs: cocaine, amphetamines,phencyclidine,methylenedioxymethamphetamine (MDMA, “ecstasy”;
look for hyperthermia, acute hepatitis, bruxism, in a college student), “bath salts”
- Environmental exposures: camphor, carbon monoxide, cyanide, methanol, organochlorides, organophosphates
- Tramadol
- Methotrexate
- Antipsychotics
- Flumazenil
- Local anesthetics
- NSAIDS
- Theophylline
Specific therapies
- Hyponatremia: hypertonic saline
- Uremia: hemodialysis
- Hepatic encephalopathy: lactulose, liver transplant
- Methanol, ethylene glycol: ethanol, fomepizole, hemodialysis
- Salicylate poisoning: sodium bicarbonate, hemodialysis
- Eclampsia: magnesium
- Thyrotoxicosis: beta blockers, propylthiouracil (PTU), iodine, radioactive iodine
- Tricyclic antidepressants: sodium bicarbonate
- Lithium: hemodialysis
- Isoniazid: pyridoxine
- Thrombotic thrombocytopenic purpura: plasma exchange
- HSV encephalitis: acyclovir
- Brain tumor: dexamethasone
- Endoscopy with small bowel biopsy (if Whipple’s disease is suspected)
Counseling
- Avoidance of driving, swimming or bathing without supervision, working at heights, etc.
References
- Theodore X. O’Connell, MD, Instant Workups: A Clinical Guide to Medicine (2008, reviewed here)
- The Merck Manual for Health Care Professionals
- Buttaravoli, Philip, MD, Minor Emergencies (2012)
- Murray, Lindsay et al, Toxicology Handbook (2011, reviewed here)

{kind=link}
Leave a Reply